Restoring Shoulder Soft Tissue Mobility in Baseball Pitchers
Shoulder and elbow injuries, especially Tommy John surgery, have been all the rage the past few years and continues to be a pain for baseball pitchers of all ages. Trust me, my 10+ years working alongside Dr. James Andrews in Birmingham were eye opening. Many kids and parents would show up expecting to have surgery, only to be told that physical therapy was their best bet to return to pitching. I applaud a surgeon who thinks physical therapy is worth a shot before going under the knife. There’s no guarantee that surgery will fix the issue and there’s no guarantee that your fastball will get any faster.
Knowing this, what can we as PT’s do to help these athletes return to their sport and prevent future episodes? My last blog post dealt with ways to improve overhead mobility and stability.
We know that the overhead athlete’s shoulder become adapted to the stresses placed upon it, especially when an adolescent is throwing around the ages of 11-14 years old.
After a pitcher throws, particularly in a game, they lose shoulder ROM. We think this is due to the eccentric forces on the back of the shoulder, causing loss of shoulder internal rotation. We showed this in a study in the American Journal of Sports Medicine.
If these soft tissue restrictions are not resolved, then the pitcher may be setting themselves up for future injury. The more I practice and research, the more I think the whole glenohumeral internal rotation deficit (GIRD) phenomenon is not as significant as we original thought. Loss of internal rotation is normal, however if they begin to lose too much and their total range of motion is reduced, the bigger risk they may have for shoulder injury. We showed this in a study back in 2011 and continue to see the trend if a pitcher’s total motion is not equal side to side when measuring the way we recommended.
Restoring Soft Tissue Mobility in Baseball Pitchers
I continue to use the supine horizontal adduction stretch with the lateral border of the shoulder blade stabilized. I find this elicits the best stretch to the back of the shoulder as long as they don’t feel a pinch in the front or the top. If so, you need to reposition and try a new angle. This is critical!
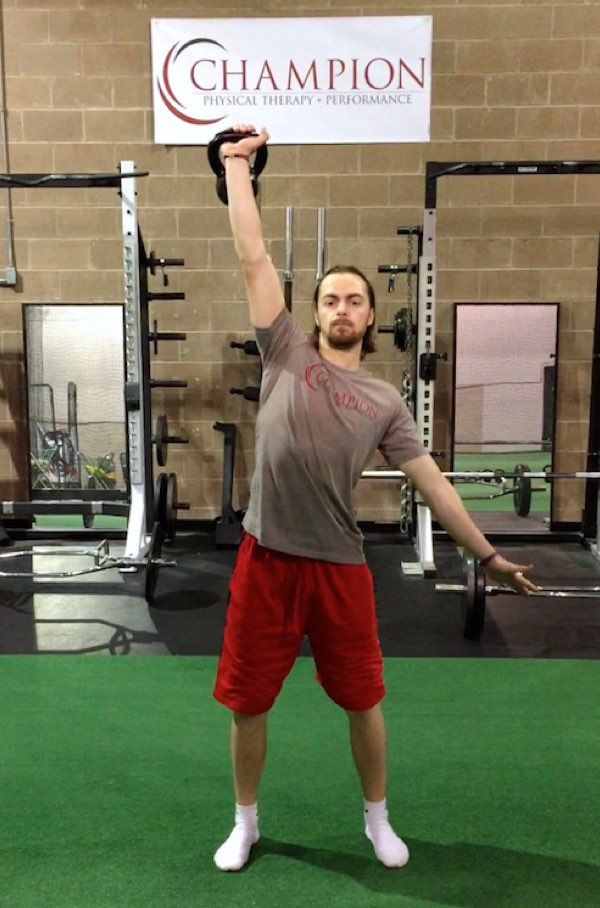
While internal rotation and GIRD get all the attention, another issue that we have noticed is loss of flexion mobility, both passive and active.
Recently, we published a study in AJSM that showed a higher elbow injury rate in the group that didn’t have full flexion range of motion. We believed ‘the correlation between shoulder flexion deficit and elbow injury in the current study may represent lack of tissue mobility and overall flexibility in injury-prone subjects.
As you can see, the dominant shoulder cannot elevate as high as the non-dominant one.

We again attribute this to soft tissue restrictions and have noticed that manual therapy on the subscapularis, pec minor, latissimus, and teres major aids in returning this motion back to normal.
Again and again I am seeing this and believe that it is critical to regain this mobility in order to continue throwing at such a high level.
Don’t rush into surgery until you have optimized your body. Significant mobility restrictions have been correlated to injury and may be the underlying cause of your actual shoulder or elbow injury. Address the true “cause” of your injury and return to throwing without surgery.